
Anatomy
The peroneus longus and brevis arise from the posterolateral surface of the fibula and the fascia of their compartment. They run over the posterior surface of the fibular tip, where there is an adaptive fibrocartilage on the fibula, with brevis next to the bone. The tendons are kept in place by the presence of a shallow groove on the posterior fibula, the superior peroneal retinaculum (SPR) which tethers the tendons to the fibula, and a fibrocatilaginous lip, which deepens the groove where it meets the retinaculum.
On the lateral surface of the calcaneum the tendons run superficial to the calcaneofibular(CFL) and lateral talocalcaneal ligaments. Tears of the CFL create a communication between the peroneal tendon sheath and the ankle – the ability of contrast to pass from one to the other is the basis of peroneal tendonography as a method of diagnosing ankle ligament rupture. Distal to the CFL the tendons run superior (brevis) and inferior (longus) to the peroneal trochlea on the lateral calcaneal wall, retained by the inferior peroneal retinaculum (IPR). Here the sheath is thickened and stenosing tenosynovitis may occur. The peroneus brevis is inserted into the inferolateral part of the tubercle of the 5 th metatarsal. The peroneus longus turns through a sharp angle to enter a fibro-osseous tunnel on the underside of the cuboid, where there is usually an accessory ossicle, the os perineum. The longus tendon inserts into the plantar surface of the first metatarsal.
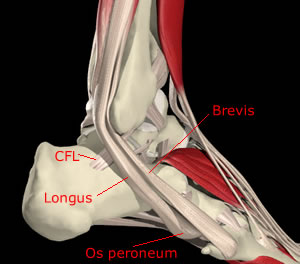
Peroneal tendons
CFL - calcaneofibular ligament
SPR - superior peroneal retinaculum
IPR - inferior peroneal retinaculum
Peroneus longus tendon passes under the foot to insert into the base of 1st metatarsal + medial cuneiform
The tendons receive blood supply from vinculae which reach them from posteriorly in the calf and usually link the two tendons. Early studies found no evidence of avascular zones(Sobel 1992), but more recent work (Petersen et al 2000) suggests relatively avascular zones in brevis at the level of the SPR, and in longus at the IPR and the sharp turn to enter the cuboid tunnel. These are the commonest levels for tears.
Function
Both tendons are plantar flexors of the ankle and evertors of the subtalar and midtarsal joints. As evertors their main opponent is tibialis posterior. In addition the peroneus longus plantarflexes the first metatarsal in opposition to tibialis anterior. Relative sparing of peroneus longus compared to tibialis anterior is probably relevant to the pathogenesis of the stiff plantarflexed first metatarsal in pes cavus. A relatively strong tibialis posterior opposed to a weaker peroneus brevis probably contributes to the development of the hindfoot varus component of cavovarus.